Clinical psychology
| Psychology |
 |
| History |
| Psychologists |
| Divisions |
|---|
| Abnormal |
| Applied |
| Biological |
| Clinical |
| Cognitive |
| Comparative |
| Developmental |
| Differential |
| Industrial |
| Parapsychology |
| Personality |
| Positive |
| Religion |
| Social |
| Approaches |
| Behaviorism |
| Depth |
| Experimental |
| Gestalt |
| Humanistic |
| Information processing |
Clinical psychology is the application of psychology to assess mental health problems, conduct and use scientific research to understand such problems, and develop, provide, and evaluate psychological care and interventions. It integrates human science, behavioral science, theory, and clinical knowledge. Central to its practice are psychological assessment, clinical formulation, and psychotherapy, although clinical psychologists also engage in research, teaching, consultation, forensic testimony, and program development and administration.
Clinical psychology is not to be confused with psychiatry, which is the medical specialty devoted to the diagnosis, prevention, and treatment of deleterious mental conditions. Psychiatrists are medical doctors who specialize in the treatment of mental disorders via a variety of methods, such as brief psychotherapy, psychoactive medications, and medical procedures such as electroconvulsive therapy (ECT), or transcranial magnetic stimulation (TMS). Additionally, psychiatrists are legally authorized to prescribe psychotropic medications, whereas this is uncommon for clinical psychologists. Although practitioners in both fields are experts in mental health, clinical psychologists are experts in psychological assessment including neuropsychological and psychometric assessment and treat mental disorders primarily through psychotherapy, generally within four primary theoretical orientations—psychodynamic, humanistic, cognitive behavioral therapy (CBT), and systems or family therapy.
Clinical psychology applies the principles and methods of psychology to prevent and relieve psychologically-based distress or dysfunction and to promote mental health and well-being. As such, this field and its practitioners provide valuable service, enabling all people to overcome psychological difficulties and live fulfilling lives both as individuals and through contributing to society as a whole.
History
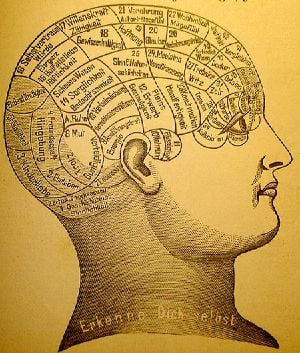
The earliest recorded approaches to assess and treat mental distress were a combination of religious, magical, and/or medical perspectives.[1] In the early nineteenth century, one approach to study mental conditions and behavior was using phrenology, the study of personality by examining the shape of the skull. Other popular treatments at that time included the study of the shape of the face (physiognomy) and Mesmer's treatment for mental conditions using magnets (mesmerism). Spiritualism and Phineas Quimby's "mental healing" were also popular.[2]
While the scientific community eventually came to reject all of these methods, academic psychologists also were not concerned with mental disorders. The study of mental illness was already included in the developing fields of psychiatry and neurology within the asylum movement.[1] It was not until the end of the nineteenth century, around the time when Sigmund Freud was first developing his "talking cure" in Vienna, that the first scientific application of clinical psychology began.
Early clinical psychology

By the second half of the 1800s, the scientific study of psychology was becoming well established in university laboratories. Although there were a few scattered voices calling for applied psychology, the general field looked down upon this idea and insisted on "pure" science as the only respectable practice.[1] This changed when Lightner Witmer (1867–1956), a past student of Wilhelm Wundt and head of the psychology department at the University of Pennsylvania, agreed to treat a young boy who had trouble with spelling. His successful treatment was soon to lead to Witmer's opening of the first psychological clinic in 1896, dedicated to helping children with learning disabilities.[3] Ten years later in 1907, Witmer was to found the first journal of this new field, The Psychological Clinic, where he coined the term "clinical psychology," defined as "the study of individuals, by observation or experimentation, with the intention of promoting change."[4]
In the early years when clinical psychology was growing, working with issues of serious mental distress remained the domain of psychiatrists and neurologists.[5] However, clinical psychologists continued to make inroads into this area due to their increasing skill at psychological assessment. Psychologists' reputation as assessment experts became solidified during World War I with the development of two intelligence tests, Army Alpha and Army Beta (testing verbal and nonverbal skills, respectively), which could be used with large groups of recruits.[2] Due in large part to the success of these tests, assessment was to become the core discipline of clinical psychology for the next quarter-century, when another war would propel the field into treatment.
Early professional organizations
The field began to organize under the name "clinical psychology" in 1917 with the founding of the American Association of Clinical Psychology. This lasted only until 1919, after which the American Psychological Association (founded by G. Stanley Hall in 1892) developed a section on Clinical Psychology, which offered certification until 1927. Growth in the field was slow for the next few years when various unconnected psychological organizations came together as the American Association of Applied Psychology in 1930, which would act as the primary forum for psychologists until after World War II when the APA reorganized. In 1945, the APA created what is now called Division 12, the Society for Clinical Psychology, which remains a leading organization in the field.[6] Psychological societies and associations in other English-speaking countries developed similar divisions, including Britain, Canada, Australia, and New Zealand.
World War II
When World War II broke out, the military once again called upon clinical psychologists. As soldiers began to return from combat, psychologists started to notice symptoms of psychological trauma labeled "shell shock" (eventually to be termed post-traumatic stress disorder) that were best treated as soon as possible. Because physicians (including psychiatrists) were over-extended in treating bodily injuries, psychologists were called on to help treat this condition.[7] At the same time, female psychologists (who were excluded from the war effort) formed the National Council of Women Psychologists with the purpose of helping communities deal with the stresses of war and giving young mothers advice on child rearing.[4] After the war, the Veterans Administration in the US made an enormous investment to set up programs to train doctoral-level clinical psychologists to help treat the thousands of veterans needing care. As a consequence, the US went from having no formal university programs in clinical psychology in 1946 to over half of all PhDs in psychology in 1950 being awarded in clinical psychology.[4] Clinical psychology in Britain developed similarly, within the context of the National Health Service, with qualifications, standards, and salaries managed by the British Psychological Society.
Doctor of Psychology degree
By the 1960s, psychotherapy had become embedded within clinical psychology, but for many, the PhD educational model did not offer the necessary training for those interested in practice rather than research. There was a growing argument that said the field of psychology in the US had developed to a degree warranting explicit training in clinical practice. The concept of a practice-oriented degree was debated in 1965 and narrowly gained approval for a pilot program at the University of Illinois starting in 1968. Several other similar programs were instituted soon after, and in 1973, at the Vail Conference on Professional Training in Psychology, the practitioner–scholar model of clinical psychology—or Vail Model—resulting in the Doctor of Psychology (PsyD) degree was recognized.[8] Although training would continue to include research skills and a scientific understanding of psychology, the intent would be to produce highly trained professionals, similar to programs in medicine, dentistry, and law. The first program explicitly based on the PsyD model was instituted at Rutgers University.[8]
A changing profession
Since the 1970s, clinical psychology has continued growing into a robust profession and academic field of study. Clinical psychologists continue to be experts in assessment and psychotherapy while expanding their focus to address issues of gerontology, sports, and the criminal justice system to name a few. One important field is health psychology, the fastest-growing employment setting for clinical psychologists in the past decade.[2] Other major changes include the impact of managed care on mental health care; an increasing realization of the importance of knowledge relating to multicultural and diverse populations; and emerging privileges to prescribe psychotropic medication.
Today, clinical psychology is defined by the Society of Clinical Psychology:
The field of Clinical Psychology involves research, teaching and services relevant to the applications of principles, methods, and procedures for understanding, predicting, and alleviating intellectual, emotional, biological, psychological, social and behavioral maladjustment, disability and discomfort, applied to a wide range of client populations. In theory, training, and practice, Clinical Psychology strives to recognize the importance of diversity and strives to understand the roles of gender, culture, ethnicity, race, sexual orientation, and other dimensions of diversity.[6]
Clinical psychologists engage in a wide range of activities. Some focus solely on research into the assessment, treatment, or cause of mental illness and related conditions. Some teach, whether in a medical school or hospital setting, or in an academic department (e.g., psychology department) at an institution of higher education. The majority of clinical psychologists engage in some form of clinical practice, with professional services including psychological assessment, provision of psychotherapy, development and administration of clinical programs, and forensics (such as providing expert testimony in a legal proceeding).[4]
In clinical practice, clinical psychologists may work with individuals, couples, families, or groups in a variety of settings, including private practices, hospitals, mental health organizations, schools, businesses, and non-profit agencies. Clinical psychologists who provide clinical services may also choose to specialize. Some specializations are codified and credentialed by regulatory agencies within the country of practice.
Clinical psychologists study a generalist program in psychology plus postgraduate training and/or clinical placement and supervision. The length of training differs across the world, ranging from four years plus post-Bachelors supervised practice to a doctorate of three to six years which combines clinical placement. The practice of clinical psychology requires a license in the United States, Canada, the United Kingdom, and many other countries.
Assessment
An important area of expertise for many clinical psychologists is psychological assessment, and there are indications that the majority, as much as 90 percent, of psychologists engage in this core clinical practice.[9] Such evaluation is usually done to gain insight into and to form a hypothesis about psychological or behavioral problems. The results of such assessments are usually used to create generalized impressions (rather than diagnosis) in service to informing treatment planning. Methods include formal testing measures, interviews, reviewing records, clinical observation, and physical examination.[10]
There exist hundreds of various assessment tools, although only a few have been shown to have both high validity (test actually measures what it claims to measure) and reliability (consistency). Many psychological assessment measures are restricted for use by those with advanced training in mental health. For instance, Pearson (one of the many companies with rights and protection of psychological assessment tools) classifies tests into several levels, with different qualifications for their use: Anybody is able to access Qualification Level A tests. Those who intend to use assessment tools at Qualification Level B must hold a master's degree in psychology, education, speech language pathology, occupational therapy, social work, counseling, or in a field closely related to the intended use of the assessment, and formal training in the ethical administration, scoring, and interpretation of clinical assessments. Those with access to Qualification C (highest level) assessment measures must hold a doctorate degree in psychology, education, or a closely related field with formal training in the ethical administration, scoring, and interpretation of clinical assessments related to the intended use of the assessment.[11]
Measurement domains
.png)
Psychological measures generally fall within one of several categories, including the following:
- Intelligence and achievement tests – These tests are designed to measure certain specific kinds of cognitive functioning (often referred to as IQ) in comparison to a norm. These tests, such as the WISC-IV and the WAIS, attempt to measure such traits as general knowledge, verbal skill, memory, attention span, logical reasoning, and visual/spatial perception. Several tests have been shown to predict accurately certain kinds of performance, especially scholastic.[9] Other tests in this category include the WRAML and the WIAT.
- Personality tests – Tests of personality aim to describe patterns of behavior, thoughts, and feelings. They generally fall within two categories: objective and projective. Objective measures, such as the MMPI, are based on restricted answers—such as yes/no, true/false, or a rating scale—which allow for the computation of scores that can be compared to a normative group. Projective tests, such as the Rorschach inkblot test, allow for open-ended answers, often based on ambiguous stimuli. Other commonly used personality assessment measures include the PAI and the NEO
- Neuropsychological tests – Neuropsychological tests consist of specifically designed tasks used to measure psychological functions known to be linked to a particular brain structure or pathway. They are typically used to assess impairment after an injury or illness known to affect neurocognitive functioning, or when used in research, to contrast neuropsychological abilities across experimental groups.
- Diagnostic Measurement Tools – Clinical psychologists are able to diagnose psychological disorders and related disorders found in the DSM-5 and ICD-10. Many assessment tests have been developed to complement the clinicians clinical observation and other assessment activities. Some of these include the SCID-IV, the MINI, as well as some specific to certain psychological disorders such as the CAPS-5 for trauma, the ASEBA, and the K-SADS for affective disorders and schizophrenia in children.
- Clinical observation – Clinical psychologists are also trained to gather data by observing behavior. The clinical interview is a vital part of the assessment, even when using other formalized tools, which can employ either a structured or unstructured format. Such assessment looks at certain areas, such as general appearance and behavior, mood and affects, perception, comprehension, orientation, insight, memory, and content of the communication. One psychiatric example of a formal interview is the mental status examination, which is often used in psychiatry as a screening tool for treatment or further testing.[9]
Diagnostic impressions
- See also: Mental disorder
After assessment, clinical psychologists may provide a diagnostic impression. Many countries use the International Statistical Classification of Diseases and Related Health Problems (ICD-10) while the US most often uses the Diagnostic and Statistical Manual of Mental Disorders. Both are nosological systems that largely assume categorical disorders diagnosed through the application of sets of criteria including symptoms and signs.
Several new models are being discussed, including a "dimensional model" based on empirically validated models of human differences (such as the five factor model of personality) and a "psychosocial model," which would take changing, intersubjective states into greater account. The proponents of these models claim that they would offer greater diagnostic flexibility and clinical utility without depending on the medical concept of illness, although they also admit that these models are not yet robust enough to gain widespread use, and should continue to be developed.[12]
Treatments
Psychotherapy involves a formal relationship between professional and client—usually an individual, couple, family, or small group—that employs a set of procedures intended to form a therapeutic alliance, explore the nature of psychological problems, and encourage new ways of thinking, feeling, or behaving.[10][13]
Clinicians have a wide range of individual interventions to draw from, often guided by their training—for example, a cognitive behavioral therapy (CBT) clinician might use worksheets to record distressing cognitions, a psychoanalyst might encourage free association, while a psychologist trained in Gestalt techniques might focus on immediate interactions between client and therapist. Clinical psychologists generally seek to base their work on research evidence and outcome studies as well as on trained clinical judgment. Although there are literally dozens of recognized therapeutic orientations, their differences can often be categorized on two dimensions: insight vs. action and in-session vs. out-session.[4]
- Insight – emphasis is on gaining a greater understanding of the motivations underlying one's thoughts and feelings (such as psychodynamic therapy)
- Action – focus is on making changes in how one thinks and acts (for example, solution focused therapy, cognitive behavioral therapy)
- In-session – interventions center on the here-and-now interaction between client and therapist (as in humanistic therapy, Gestalt therapy)
- Out-session – a large portion of therapeutic work is intended to happen outside of session (for example, bibliotherapy, rational emotive behavior therapy)
The methods used are also different in regards to the population being served as well as the context and nature of the problem. Therapy will look very different for a traumatized child, a depressed but high-functioning adult, a group of people recovering from Substance abuse, and a ward of the state suffering from terrifying delusions. Other elements that play a critical role in the process of psychotherapy include the environment, culture, age, cognitive functioning, motivation, and duration (brief or long-term therapy).[13]
Four main schools
Many clinical psychologists are integrative or eclectic and draw from the evidence base across different models of therapy in an integrative way, rather than using a single specific model.
In the UK, clinical psychologists have to show competence in at least two models of therapy, including CBT, to gain their doctorate. The British Psychological Society Division of Clinical Psychology has been vocal about the need to follow the evidence base rather than being wedded to a single model of therapy.
In the US, intervention applications and research are dominated in training and practice by essentially four major schools of practice: psychodynamic, humanism, behavioral/cognitive behavioral, and systems or family therapy.[10]
Psychodynamic
The psychodynamic perspective developed out of the psychoanalysis of Sigmund Freud. The core object of psychoanalysis is to make the unconscious conscious—to make the client aware of his or her own primal drives (namely those relating to sex and aggression) and the various defenses used to keep them in check.[13] The essential tools of the psychoanalytic process are the use of free association and an examination of the client's transference towards the therapist, defined as the tendency to take unconscious thoughts or emotions about a significant person (such as a parent) and "transfer" them onto another person. Major variations on Freudian psychoanalysis practiced today include self psychology, ego psychology, and object relations theory. These general orientations now fall under the umbrella term "psychodynamic psychology," with common themes including examination of transference and defenses, an appreciation of the power of the unconscious, and a focus on how early developments in childhood have shaped the client's current psychological state.[13]
Humanistic/Experiential
Humanistic psychology was developed in the 1950s in reaction to both behaviorism and psychoanalysis, largely due to the person-centered therapy of Carl Rogers (often referred to as Rogerian Therapy) and existential psychology developed by Viktor Frankl and Rollo May.[10] Rogers believed that a client needed only three things from a clinician to experience therapeutic improvement—congruence, unconditional positive regard, and empathetic understanding.[14] By using phenomenology, intersubjectivity, and first-person categories, the humanistic approach seeks to get a glimpse of the whole person and not just the fragmented parts of the personality.[15] According to humanistic thinking, each individual person already has inbuilt potentials and resources that might help them to build a stronger personality and self-concept.[16] The mission of the humanistic psychologist is to help the individual employ these resources via the therapeutic relationship.
Emotionally focused therapy (EFT) was initially informed by humanistic–phenomenological and Gestalt theories of therapy:
Emotion Focused Therapy can be defined as the practice of therapy informed by an understanding of the role of emotion in psychotherapeutic change. EFT is founded on a close and careful analysis of the meanings and contributions of emotion to human experience and change in psychotherapy. This focus leads therapist and client toward strategies that promotes the awareness, acceptance, expression, utilization, regulation, and transformation of emotion as well as corrective emotional experience with the therapist. The goals of EFT are strengthening the self, regulating affect, and creating new meaning.[17]
Behavioral therapy and CBT
.jpg)
Behavior therapy (or Behavioral therapy) has a rich tradition, with roots in behaviorism. In behavior therapy, environmental events predict the way we think and feel. Our behavior sets up conditions for the environment to feedback back on it. Sometimes the feedback reinforces the behavior which leads it to increase, and sometimes punishment follows which decreases the frequency of the behavior. Multiple assessment techniques have come from this approach including functional analysis (psychology), which has found a strong focus in the school system. In addition, multiple intervention programs have have been developed, including community reinforcement approach for treating addictions, acceptance and commitment therapy, functional analytic psychotherapy, including dialectic behavior therapy and behavioral activation, as well as specific techniques including contingency management and exposure therapy.
In the 1950s and 1960s, theorists Albert Ellis and Aaron T. Beck independently began combining the perspectives of Cognitive psychology and Behaviorism to create Cognitive Behavioral Therapy (CBT). Essentially, it is based on the idea that how we think (cognition), how we feel (emotion), and how we act (behavior) interact together. Thus, certain thoughts or ways of interpreting the world (called schemas) can cause emotional distress or result in behavioral problems. The object of CBT is to discover the biased and irrational thinking that leads to emotional problems and to help the client take control over his or her thinking processes in such a way that will lead to increased well-being.[18] There are many techniques used, such as systematic desensitization, socratic questioning, and keeping a cognition observation log. Modified approaches that fall into the category of CBT have also developed, including dialectic behavior therapy and mindfulness-based cognitive therapy. Similar approaches, such as Rational Emotive Behavior Therapy and Dialectic Behavior Therapy, have been shown to be effective in treating certain conditions, such as depression and phobias.
Systems or family therapy
Systems or family therapy works with couples and families, and emphasizes family relationships as an important factor in psychological health. The central focus tends to be on interpersonal dynamics, especially in terms of how change in one person will affect the entire system.[19] Therapy is therefore conducted with as many significant members of the "system" as possible. Goals can include improving communication, establishing healthy roles, creating alternative narratives, and addressing problematic behaviors.
Other therapeutic perspectives
There exist dozens of recognized schools or orientations of psychotherapy—the list below represents a few influential orientations not given above. Although they all have some typical set of techniques practitioners employ, they are generally better known for providing a framework of theory and philosophy that guides a therapist in his or her working with a client.
- Existential – Existential psychotherapy postulates that people are largely free to choose who we are and how we interpret and interact with the world. It intends to help the client find deeper meaning in life and to accept responsibility for living. As such, it addresses fundamental issues of life, such as death, loneliness, and freedom. The therapist emphasizes the client's ability to be self-aware, freely make choices in the present, establish personal identity and social relationships, create meaning, and cope with the natural anxiety of living.[20]
- Gestalt – Gestalt therapy was primarily founded by Fritz Perls in the 1950s. This therapy is perhaps best known for using techniques designed to increase self-awareness, the best-known being the "empty chair technique." Such techniques are intended to explore resistance to "authentic contact," resolve internal conflicts, and help the client complete "unfinished business."[21]
- Transpersonal – The transpersonal perspective places a stronger focus on the spiritual facet of human experience.[22] Transpersonal psychology is concerned with helping clients achieve their highest potential through helping explore spirituality and/or transcendent states of consciousness.
- Feminism – Feminist therapy is an orientation arising from the disparity between the origin of most psychological theories (which have male authors) and the majority of people seeking counseling being female. It focuses on societal, cultural, and political causes and solutions to issues faced in the counseling process. It openly encourages the client to participate in the world in a more social and political way.[23]
- Positive psychology – Positive psychology is the scientific study of human happiness and well-being, which started to gain momentum in 1998 due to the call of Martin Seligman, then president of the APA. The history of psychology shows that the field has been primarily dedicated to addressing mental illness rather than mental wellness. Applied positive psychology's main focus, therefore, is to increase one's positive experience of life and ability to flourish by promoting such things as optimism about the future, a sense of flow in the present, and personal traits like courage, perseverance, and altruism.[24] There is empirical evidence to show that by promoting Seligman's three components of happiness—positive emotion (the pleasant life), engagement (the engaged life), and meaning (the meaningful life)—positive therapy can decrease clinical depression.[25]
Criticisms and controversies
Clinical psychology is a diverse field and there have been recurring tensions over the degree to which clinical practice should be limited to treatments supported by empirical research.[26] Despite some evidence showing that all the major therapeutic orientations are about of equal effectiveness, there remains much debate about the efficacy of various forms treatment in use in clinical psychology.[27]
Notes
- ↑ 1.0 1.1 1.2 Ludy T. Benjamin Jr., A Brief History of Modern Psychology (Wiley-Blackwell, 2006, ISBN 978-1405132053).
- ↑ 2.0 2.1 2.2 Ludy T. Benjamin Jr., "A history of clinical psychology as a profession in America (and a glimpse at its future)." Annual Review of Clinical Psychology 1(1) (2005): 1–30.
- ↑ P. McReynolds, "Lightner Witmer. Little-known founder of clinical psychology." American Psychologist 42(9) (1987): 849–858.
- ↑ 4.0 4.1 4.2 4.3 4.4 Bruce E. Compas and Ian H. Gotlib, Introduction to Clinical Psychology: Science and Practice (McGraw-Hill College, 2001, ISBN 978-0070124912).
- ↑ Donald K. Routh, Clinical Psychology Since 1917: Science, Practice, and Organization (Springer, 2013, ISBN 978-1475797145).
- ↑ 6.0 6.1 Society of Clinical Psychology APA. Retrieved September 28, 2023.
- ↑ John M. Reisman, A History of Clinical Psychology (Taylor & Francis, 1991, ISBN 978-1560321880).
- ↑ 8.0 8.1 Bridget Murray, The degree that almost wasn't: The PsyD comes of age Monitor on Psychology 31(1) (2000): 52. Retrieved September 28, 2023.
- ↑ 9.0 9.1 9.2 Gary Groth-Marnat and A. Jordan Wright, Handbook of Psychological Assessment (Hoboken, NJ: John Wiley & Sons, 2016, ISBN 978-1118960646).
- ↑ 10.0 10.1 10.2 10.3 Thomas G. Plante, Contemporary Clinical Psychology. New York: Wiley, 2020, ISBN 978-1119706311).
- ↑ Qualifications policy Pearsons. Retrieved September 29, 2023.
- ↑ W. Edward Craighead and Charles B. Nemeroff (eds.), The Corsini Encyclopedia of Psychology and Behavioral Science (Wiley, 2000, ISBN 978-0471240983).
- ↑ 13.0 13.1 13.2 13.3 Glen O. Gabbard, Psychodynamic Psychiatry in Clinical Practice (Washington, DC: American Psychiatric Press, 2014, ISBN 978-1585624430).
- ↑ Michael McMillan, The Person-Centred Approach to Therapeutic Change (SAGE Publications Ltd, 2004, ISBN 978-0761948698).
- ↑ John Rowan, Ordinary Ecstasy: The Dialectics of Humanistic Psychology (Routledge, 2001, ISBN 978-0415236331).
- ↑ Kirk J. Schneider, James F. T. Bugental, and J. Fraser Pierson (eds.), The Handbook of Humanistic Psychology: Leading Edges in Theory, Research, and Practice (SAGE Publications, Inc, 2002, ISBN 978-0761927822).
- ↑ Leslie S. Greenberg, Emotion-Focused Therapy (American Psychological Association, 2016, ISBN 978-1433826306).
- ↑ Aaron T. Beck, Denise D. Davis, and Arthur Freeman(eds.), Cognitive Therapy of Personality Disorders (New York: Guilford Press, 2015, ISBN 978-1462525812).
- ↑ Gerald Corey, Theory and Practice of Counseling and Psychotherapy (Brooks Cole, 2000, ISBN 978-0534348236).
- ↑ Emmy van Deurzen, Existential Counseling & Psychotherapy in Practice (SAGE Publications Ltd, 2012, ISBN 978-1849200684).
- ↑ Ansel L. Woldt and Sarah M. Toman, Gestalt Therapy: History, Theory, and Practice (SAGE Publications, Inc, 2005, ISBN 978-0761927914).
- ↑ Seymour Boorstein (ed.), Transpersonal Psychotherapy (Albany: State University of New York Press, 1996, ISBN 978-0791428351)
- ↑ Marcia Hill and Mary Ballou (eds.), The Foundation and Future of Feminist Therapy (New York: Routledge, 2005, ISBN 978-0789002174).
- ↑ C.R. Snyder and Shane J. Lopez (eds.), Handbook of Positive Psychology (Oxford University Press, 2001, ISBN 978-0195135336).
- ↑ Martin E.P. Seligman, Tayyab Rashid, and Acacia C. Parks, Positive Psychotherapy American Psychologist 61(8) (2006): 774–788. Retrieved September 29, 2023.
- ↑ David Pilgrim and Andrew Treacher, Clinical Psychology Observed (Routledge, 1992, ISBN 978-0415046329).
- ↑ Scott O. Lilienfeld, Steven Jay Lynn, and Jeffrey M. Lohr (eds.), Science and Pseudoscience in Clinical Psychology (New York: Guilford Press, 2014, ISBN 978-1462517510).
ReferencesISBN links support NWE through referral fees
- Beck, Aaron T., Denise D. Davis, and Arthur Freeman(eds.). Cognitive Therapy of Personality Disorders. New York: Guilford Press, 2015. ISBN 978-1462525812
- Benjamin, Ludy T. Jr. A Brief History of Modern Psychology. Wiley-Blackwell, 2006 ISBN 978-1405132053
- Boorstein, Seymour (ed.). Transpersonal Psychotherapy. Albany: State University of New York Press, 1996. ISBN 978-0791428351
- Compas, Bruce E., and Ian H. Gotlib. Introduction to Clinical Psychology: Science and Practice. McGraw-Hill College, 2001. ISBN 978-0070124912
- Corey, Gerald. Theory and Practice of Counseling and Psychotherapy. Brooks Cole, 2000. ISBN 978-0534348236
- Craighead, W. Edward, and Charles B. Nemeroff (eds.). The Corsini Encyclopedia of Psychology and Behavioral Science. Wiley, 2000. ISBN 978-0471240983
- van Deurzen, Emmy. Existential Counseling & Psychotherapy in Practice. SAGE Publications Ltd, 2012. ISBN 978-1849200684
- Gabbard, Glen O. Psychodynamic Psychiatry in Clinical Practice. Washington, DC: American Psychiatric Press, 2014. ISBN 978-1585624430
- Greenberg, Leslie S. Emotion-Focused Therapy. American Psychological Association, 2016. ISBN 978-1433826306
- Groth-Marnat, Gary, and A. Jordan Wright. Handbook of Psychological Assessment. Hoboken, NJ: John Wiley & Sons, 2016. ISBN 978-1118960646
- Hill, Marcia, and Mary Ballou (eds.). The Foundation and Future of Feminist Therapy. New York: Routledge, 2005. ISBN 978-0789002174
- Lilienfeld, Scott O., Steven Jay Lynn, and Jeffrey M. Lohr (eds.). Science and Pseudoscience in Clinical Psychology. New York: Guilford Press, 2014. ISBN 978-1462517510
- McMillan, Michael. The Person-Centred Approach to Therapeutic Change. SAGE Publications Ltd, 2004. ISBN 978-0761948698
- Pilgrim, David, and Andrew Treacher. Clinical Psychology Observed. Routledge, 1992. ISBN 978-0415046329
- Plante, Thomas G. Contemporary Clinical Psychology. New York: Wiley, 2020. ISBN 978-1119706311
- Reisman, John M. A History of Clinical Psychology. Taylor & Francis, 1991. ISBN 978-1560321880
- Routh, Donald K. Clinical Psychology Since 1917: Science, Practice, and Organization. Springer, 2013. ISBN 978-1475797145
- Schneider, Kirk J., James F. T. Bugental, and J. Fraser Pierson (eds.). The Handbook of Humanistic Psychology: Leading Edges in Theory, Research, and Practice. SAGE Publications, Inc, 2002. ISBN 978-0761927822
- Snyder, C.R., and Shane J. Lopez (eds.). Handbook of Positive Psychology. Oxford University Press, 2001. ISBN 978-0195135336
- Woldt, Ansel L., and Sarah M. Toman. Gestalt Therapy: History, Theory, and Practice. SAGE Publications, Inc, 2005. ISBN 978-0761927914
External links
All links retrieved January 7, 2024.
- American Academy of Clinical Psychology
- American Association for Marriage and Family Therapy
- American Board of Professional Psychology
- Annual Review of Clinical Psychology
- APA Society of Clinical Psychology (Division 12)
- Association of State and Provincial Psychology Boards (ASPPB)
- NAMI: National Alliance on Mental Illness
- National Institute of Mental Health
Credits
New World Encyclopedia writers and editors rewrote and completed the Wikipedia article in accordance with New World Encyclopedia standards. This article abides by terms of the Creative Commons CC-by-sa 3.0 License (CC-by-sa), which may be used and disseminated with proper attribution. Credit is due under the terms of this license that can reference both the New World Encyclopedia contributors and the selfless volunteer contributors of the Wikimedia Foundation. To cite this article click here for a list of acceptable citing formats.The history of earlier contributions by wikipedians is accessible to researchers here:
The history of this article since it was imported to New World Encyclopedia:
Note: Some restrictions may apply to use of individual images which are separately licensed.